Good afternoon.
I am a new member of this group and a newly identified sufferer. I am 71 years old, reasonably fit, hypertension controlled by drugs.
I am looking for advice at a level I can understand, and I hope for some re-assurance.
My journey so far is this:
Feb-March 2022 raised PSA level over 2 tests (can't remember the exact amount, but 6-ish).
DRE not suspicious, referred Urology, MRI Scan. Advised scan clear and not to worry unless PSA reached 10-12.
Found out recently that something was present at PIRADS 2. Not regarded as clinically significant.
No PSA test in 2023 - both myself and my doctors failed on that, to my bitter regret.
This year, I asked for a test in February - I noticed that I hadn't had one.
Three tests undertaken:
Referral to Urology.
20/04/2024 Appointment with Urology. DRE "nothing suspicious" referred MRI
30/04/2024 informed results of scan. Quote - "Two foci of clinically significant tumour in right peripheral peripheral zone at the neurovascular bundle and left seminal vesicle, PIRADS 5. There is a right pelvic sidewall metastic lymph node measuring 13mm in the short axis. Therefore T3b N1 MX multifocal prostatic tumour."
I sort of understood sone of this.
07/05/2024 - CT Scan
07/05/2024 - Bone Scan
23/05/2024 - Biopsy carried out. Results to above scan reported to myself and GP
In view of what happens next, these things may be important.
All my searching of MacMillan and Prostrate Cancer suggested that a staging of T3b N1 MX (the original note) should be, with only a local lymph node (in the pelvic area) be called either "Locally Advanced" or "Advanced Localised".
07/06/2023 - meeting with specialist nurse to cover biopsy results. I expected more of a plan from this meeting than I got, but I think that was my fault.
Results - Gleason Score 9 therefore CPG 5. 31 Cores in biopsy, 12 Positive - 10 Gleason 9, 2 Gleason 2. Not the reults I would have liked.
Encouraging statements "you're not going anywhere" "this treatment will stop it dead in its tracks".
Overall discussion not too encouraging by way of answers. I will be given (to follow) an appointment with a Consultant Oncologist. Apparently I have to wait for further answers from the consultant.
Nurse did not describe the results in any kind of way I recognised, whilst agreeing with att the staging details etc. Just referred to "metastasised" but still only referring to the details above. They gave me this website - www.canceralliance.co.uk/prostate - to "know my options".
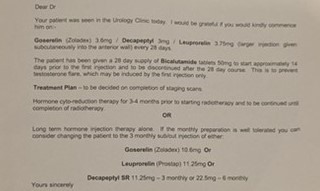
This gives a page which quotes all the same treatment options as for locally advanced prostate cancer, but without saying that. It says that, untreated, the prognosis is very poor - but that is no longer the case. The letter imaged below shows the treatment currently in place, which I have started.
My problem now is that I don't have much confidence and don't know what to ask the consultant, and, if necessary, badger him for further referrals.
My research has now reached the stage of more confusion than comfort.
So, my questions are twofold:
Just a word, I am feeling a bit shaky at the moment since my further research is just getting too complex. Please be as encouraging as is still useful. I also plan to speak to the Prostate Cancer UK specialist nurses on Wednesday (I have a part-time job).








