My wife's pathology indicates:
ER+8
Projesterone positive
Grade 2
HER2+ with FISH TEST arranged
Lump 11 mm on ultrasound and 15mm on mammogram
I don't understood how good or bad this overall pathology is! One doctor said the outlook was excellent.
The surgeon to be, is postponing surgery for at least 3 months due to C.V. (and who knows thereafter) and prescribing an AI. This implies surgery is not too urgent. However, I found that another hospital is prioritising HER2 patients.! I am a little confused. Why has the surgeon to be, come up with a treatment plan ie no surgery and an AI when the FISH results are a week away?
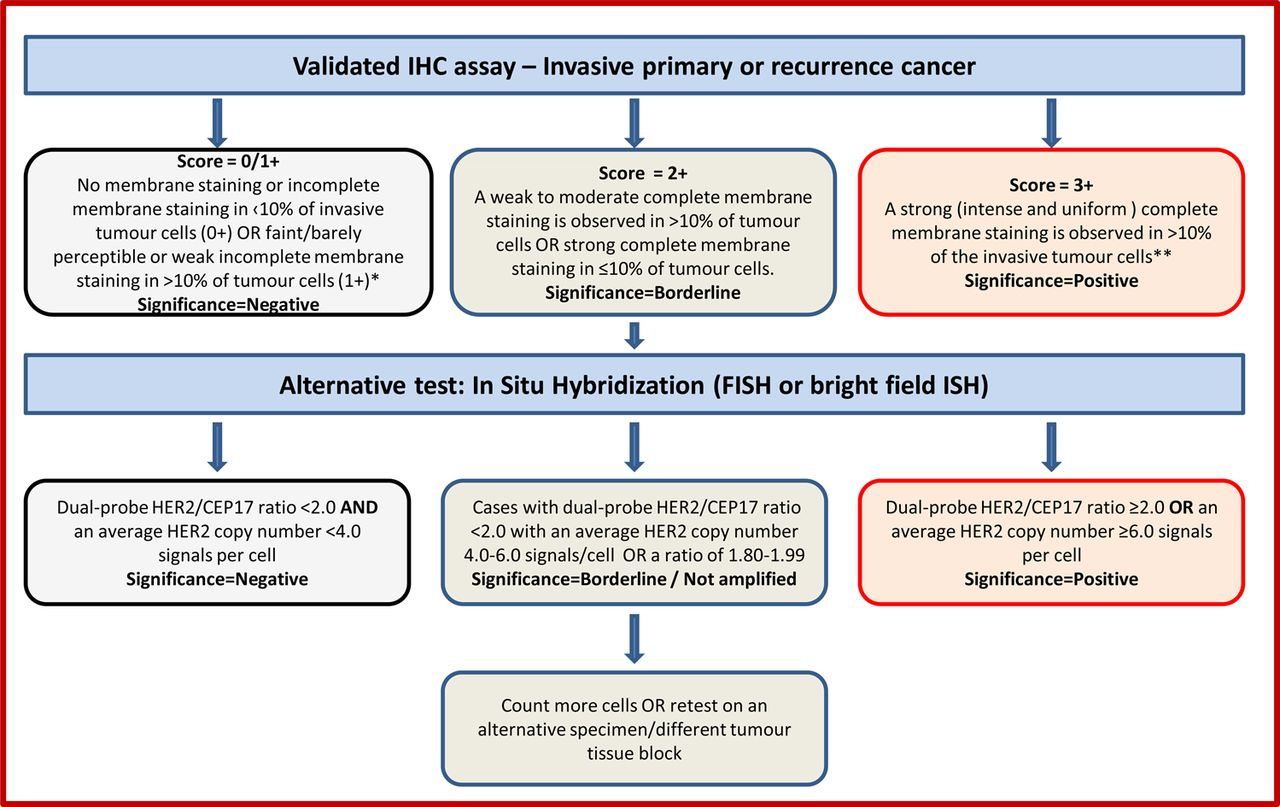
From my reading I note that HER2+ is considered borderline so a FISH TEST is necessary ie
"The IHC test uses a chemical dye to stain the HER2 proteins. The IHC gives a score of 0 to 3+ that measures the amount of HER2 proteins on the surface of cells in a breast cancer tissue sample. If the score is 0 to 1+, it’s considered HER2-negative. If the score is 2+, it's considered borderline. A score of 3+ is considered HER2-positive. If the IHC test results are borderline, it’s likely that a FISH test will be done on a sample of the cancer tissue to determine if the cancer is HER2-positive".
What is HER2 borderline? Can the result be NO HER2, or is there only HER positive or negative? How serious or not is all this? I am getting conflicting feedback!
What are the treatment implications?
Anyone with direct experience of this puzzler who can explain it to me?
D