
One of the most controversial aspects of Neuroendocrine Tumours (NETs) is the ‘benign vs malignant’ question. It’s been widely debated and it frequently patrols the various patient forums and other social media platforms. It raises emotions and it triggers many responses ….. at least from those willing to engage in the conversation. At best, this issue can cause confusion, particularly to those who thought they had a handle on it. At worst, it might contradict what new patients have been told by their physicians (….or not been told). For some, it could cause some great concern and worry. In many ways, this topic is similar to the debate I raised in my blog ‘Incurable vs Terminal’. You may benefit from reading this blog before you move on.
To fully understand this issue, I’d like to cover some basic but widely accepted definitions of cancer. I also need to bring the ‘C’ word into the equation (Carcinoid), because the history of these tumours is frequently where a lot of the confusion lies. Let’s look at these definitions provided by the National Cancer Institute. I could have selected a number of organisations but in general, they all tend to agree with these definitions give or take a few words. I supply these widely accepted definitions because there is an associated ‘tumour’ vs ‘cancer’ debate too.
Cancer – Cancer is the name given to a collection of related diseases. In all types of cancer, some of the body’s cells begin to divide without stopping and spread into surrounding tissues. There are more than 100 types of cancer which are usually named for the organs or tissues where the cancers form. However, they also may be described by the type of cell that formed them.
Author’s note: The last sentence is important for Neuroendocrine Tumour awareness (i.e. Neuroendocrine Tumour of the Pancreas rather than Pancreatic Cancer).
Carcinoma – Carcinomas are the most common grouping of cancer types. They are formed by epithelial cells, which are the cells that cover the inside and outside surfaces of the body. There are many types of epithelial cells, which often have a column-like shape when viewed under a microscope.
Author’s note: High Grade (or Grade 3) NETs are deemed to be a ‘Carcinoma’ according to the most recent World Health Organisation (WHO) classification of Neuroendocrine Tumours (2010). You will have heard of some of the types of Carcinoma such as ‘Adenocarcinoma’ (incidentally, the term ‘Adeno’ simply means ‘gland’).
Malignant – Cancerous. Malignant cells can invade and destroy nearby tissue and spread to other parts of the body.
Benign – Not cancerous. Benign tumors may grow larger but do not spread to other parts of the body.
Tumour (Tumor) – An abnormal mass of tissue that results when cells divide more than they should or do not die when they should. Tumors may be benign (not cancerous), or malignant (cancerous). Also called Neoplasm.
Author’s Note: Neoplasm is interesting as this is the term frequently used by ENETS and NANETS in their technical documentation, sometimes as a term to cover all Neuroendocrine Grades (Tumour and Carcinoma).
Definitions out of the way, I have studied the UKINETS and NANETS guidance both of which are based on internationally recognised classification schemes (i.e. the World Health Organisation (WHO)). Note: The ENETS guidance for 2016 is by paid subscription and the older versions are not wholly suitable for this task but I’ve been able to find European references with extracts, particularly with interpretations of the WHO classification schemes. I will update this blog (if necessary) once I’m able to access the ENETS 2016 documents. The latest WHO iteration is from 2010 and I’m fairly certain, having studied extracts from various European references, that the statements below will be covered within the most recent ENETS documentation.
In older versions of the WHO classification schemes (1980 and 2000), the words ‘benign’ and ‘uncertain behaviour’ were used for Grades 1 and 2. However, in the 2010 edition, the classification is fundamentally different. Firstly, it separated out grade and stage for the first time (stage would now be covered by internationally accepted staging systems such as TNM – Tumour, (Lymph) Nodes, Metastasis). Additionally, and this is key to the benign vs malignant discussion, the WHO 2010 classification is based on the concept that all NETs have malignant potential. Here’s a quote from the UKINETS Guidelines in 2011 (Ramage, Caplin, Meyer, Grossman, et al)
Tumours should be classified according to the WHO 2010 classification (Bosman FT, Carneiro F, Hruban RH, et al. WHO Classification of Tumours of the Digestive System. Lyon: IARC, 2010). This classification is fundamentally different from the WHO 2000 classification scheme, as it no longer combines stage related information with the two-tiered system of well and poorly differentiated NETs. The WHO 2010 classification is based on the concept that all NETs have malignant potential, and has therefore abandoned the division into benign and malignant NETs and tumours of uncertain malignant potential.
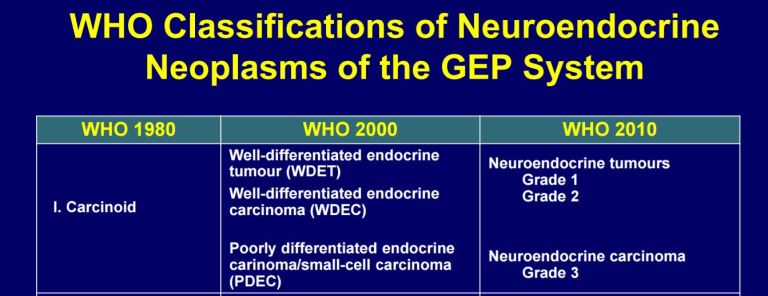
A comparison of WHO NET Classifications 1980-2000-2010 (Source ESMO)
Let me first explain that I’m talking about Carcinoid as a type of NET and not using it to mean all NETs (clearly what would be incorrect). I’m specifically mentioning it as a standalone type of NET because I believe this is where some of the confusion starts. History lesson – Carcinoid tumours were first identified as a specific, distinct type of growth in the mid-1800’s, and the name “carcinoid” was first applied in 1907 by Oberndorfer in Europe in an attempt to designate these tumors as midway between carcinomas (cancers) and adenomas (benign tumors). The word ‘Carcinoid’ originates from the term ‘Carcinoma-like’. ‘CARCIN’ is a truncation of Carcinoma (by definition cancerous or malignant tumour). ‘OID’ is a suffix used in medical parlance meaning ‘resembling’ or ‘like’. According to Dr Richard Warner, there are a few types of growths that are sort of midway between these two classifications of benign and malignant. Carcinoid tumors are the most often occurring of these rare types of “midway” growths. However, he has said in this video (start at 2 minutes) “they (Carcinoid) are cancers, they don’t all fulfil their malignant potential, but they all have that possible outcome”. He therefore agrees with the UKINETS interpretation of the WHO classification above (at least for the type of NETs called Carcinoid Tumours). Read more from Dr Warner here.
If you read any NET support website it will normally begin by stating that Neuroendocrine Tumours constitute a heterogeneous group of tumours. This means they are a wide-ranging group of different types of tumours. However, the latest WHO classification scheme uses the terms ‘Neuroendocrine Tumour’ for well differentiated Grade 1 (low-grade) and Grade 2 (Intermediate Grade); and ‘Neuroendocrine Carcinoma’ for Grade 3 or poorly differentiated tumours. Note there are one or two exceptions but the detail would cloud the aim of this blog. Based on the quote above, my interpretation is that Grade 1 is a low-grade malignancy and so on. You may benefit from reading my blog on Staging and Grading of NETs as this is also a poorly understood area.
By any accepted definition of cancer terms, a tumour can be non-cancerous (benign) or cancerous (malignant). This is correct for any cancer type. I’m sure it’s therefore possible that a benign Neuroendocrine Tumour can be present in certain scenarios. For example, the word is used in the 2016 version of Inter Science Institute publication on Neuroendocrine Tumors, a document I frequently reference in my blog. For example, I’ve seen statements such as “These tumors are most commonly benign (90%)” in relation to Insulinoma (a type of Pancreatic NET or pNET). Ditto for Pheochromocytoma (an adrenal gland NET). Pituitary ‘adenomas’ are by definition benign (adenoma is the benign version of Adenocarcinoma). And I note that there is a ‘benign’ code option for every single NET listed in the WHO International Classification of Diseases (ICD) system.
Here’s an interesting piece of information from NET expert Dr Matthew Kulke who was referring to Carcinoid Tumours discovered on autopsy and said “……..the incidence in autopsy series is four times higher, eight per hundred thousand population per year. What this indicates is that carcinoid tumors very often have a slow and indolent clinical course. In fact, probably more people die with carcinoid tumors than of carcinoid tumors. This is an important distinction that really makes carcinoid tumors and other endocrine tumors very different from the other types of cancer we typically hear about.” That got me thinking about the scenario where asymptomatic, small, localised, benign NETs are discovered by accident. It’s a tough call for any doctor (there’s a useful video linked below which emphasises this – See Dr Lowell Anthony video below). That said, it also got me thinking about the fact that many of these patients perhaps had comorbidities and vague symptoms but were never assessed properly. It also confirms something I keep repeating – NETs are not rare.
That leads me nicely into the well-known fact that benign tumours can still cause problems if they grow very large and start to invade or press on other body organs. Many NETs release hormones that produce (say) endocrine system issues and so treatment and/or surveillance are/is often still required. It’s also possible that a benign tumour could eventually turn cancerous (malignant) and this may lead to further medical decisions or courses of action.
I’m sure this is no different to many other cancers. We all know someone who has had a ‘cancer scare’ right? They go for checks, they take a biopsy and it’s found to be nothing of worry. I’ve seen this many times with friends who had a scare with many different types of cancer.
There’s a reason why the WHO declared in 2010 that all NETs have malignant potential. It may not happen or it may happen slowly over time but as Dr Warner says, they don’t all fulfill their malignant potential, but they all have that possible outcome. Thus why ongoing surveillance is important after any diagnosis of Neuroendocrine Tumour of any grade or at any stage. Dr Lowell Anthony, a NET Specialist from the University of Kentucky explains this much better than I can – CLICK HERE to hear his two-minute video clip.
This was a difficult piece of research. However, based on the above, use of the word ‘benign’ is probably best used with care given the 2010 WHO classification of NETs. Also I would certainly (at least) raise an eyebrow if someone said to anyone with any NET tumour, “you don’t need any treatment or surveillance for a NET”; or “it has been cured and no further treatment or surveillance is required”. Particularly if they are not a NET specialist or a recognised NET Centre.
Remember, I’m not a medical professional, so if you are in any doubt as to the status of your NET, you should discuss this directly with your specialist. A good place to start is evidence of your Grade and Stage.
Thanks for listening
Ronny
Hey Guys, I’m also active on Facebook. Like my page for even more news.







