This is the second blog in the Neuroendocrine Cancer Nutrition series. In Blog 1, I focussed on Vitamin and Mineral deficiency risks for patients. Those who remember the content will have spotted the risks pertaining to the inability to absorb particular vitamins and minerals. This comes under the general heading of Malabsorption and in Neuroendocrine Cancer patients, this can be caused or exacerbated by one or more of a number of factors. It's worth pointing out that malabsorption issues can be caused by many other reasons. However, it is possible that malabsorption and nutrient deficiency issues can form part of the presentational symptoms which eventually lead to a diagnosis of Neuroendocrine Cancer; e.g. in my own case, I was initially diagnosed with Iron Deficiency Anaemia.
Crash Course....... We eat food, but our digestive system doesn’t absorb food, it absorbs nutrients. Food has to be broken down from things like steak and broccoli into its nutrient pieces: amino acids (from proteins), fatty acids and cholesterol (from fats), and simple sugars (from carbohydrates), as well as vitamins, minerals, and a variety of other plant and animal compounds. Digestive enzymes, primarily produced in the pancreas and small intestine (they’re also made in saliva glands and the stomach), break down our food into nutrients so that our bodies can absorb them. If we don’t have enough digestive enzymes, we can’t break down our food—which means even though we’re eating well, we aren’t absorbing all that good nutrition.
The malabsorption associated with Neuroendocrine Cancer is most prevalent with the inability to digest fat properly which can lead to steatorrhea. Patients will recognise this in their stools. They may be floating, foul-smelling and greasy (oily) and frothy looking. Whilst we all need some fat in our diets (e.g. for energy), if a patient is not absorbing fat, it ends up being wasted in their stools and in addition to the steatorrhea, it can also potentially lead to (unwanted) weight loss and micronutrient deficiencies of the fat soluble vitamins A, D, E and K. Certain water-soluble vitamins, particularly B3 and B12, are also at risk.
Surgery can play a big part in malabsorption issues.
If a patient has undergone Pancreatic surgery, this will most likely effect the availability of pancreatic digestive enzymes needed to break down food.
Many Small Intestine NET (SINET) patients will suffer due to the removal of sections of their ileum, an area where absorption of water-soluble vitamins and other nutrients take place. In fact, the terminal ileum is really the only place where B12 is efficiently absorbed. Although a less common tumour location, jejunum surgery could result in loss of nutrients as this section of the small intestine is active in digestive processes. Malabsorption issues for SINETs are an added complication to the issues caused by a shorter bowel (e.g. increased transit times).
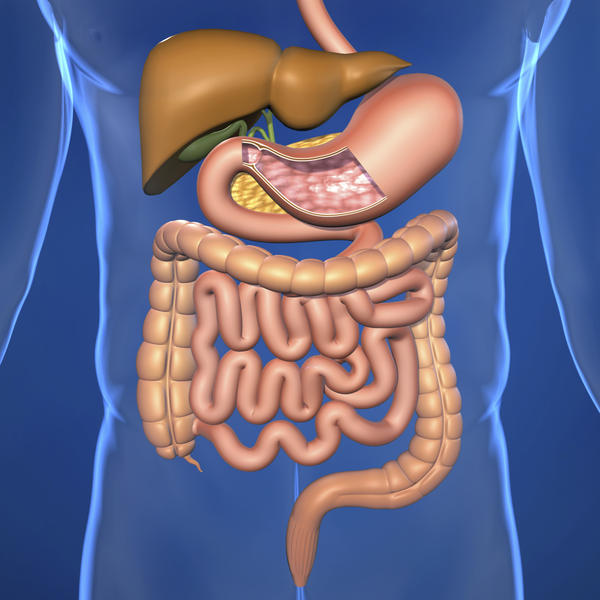
The Gallbladder plays an important part in the digestive system - particularly in fat breakdown. One of the key side effects of Somatostatin Analogues (Octreotide and Lanreotide) is the formation of gall stones and many Neuroendocrine Cancer patients have their gallbladder removed to offset the risk of succumbing to these issues downstream. The liver continually manufactures bile, which travels to the gallbladder where it is stored and concentrated. Bile helps to digest fat and the gallbladder automatically secretes a lot of bile into the small intestine after a fatty meal. However, when the gallbladder is removed, the storage of bile is no longer possible and to a certain extent, neither is the 'on demand automation'. This results in the bile being constantly delivered/trickled into the small intestine making the digestion of fat less efficient. Any issues with Bile Ducts can also have a similar effect.
The Liver has multiple functions including the production of bile as stated above. However, one of its key functions within the digestive system is to process the nutrients absorbed from the small intestine. If this process is affected by disease, it can potentially worsen the issues outlined above.
Somatostatin Analogues can also have an effect on the ability to digest fat as they inhibit the production of pancreatic digestive enzymes - this is a listed side effect of both.
Summary
Steatorrhea issues can be addressed by prescribing enzyme replacement products as directed by your doctors or dietician. The levels of the fat soluble vitamins (ADEK) and B vitamins such as B12, need to be monitored through testing and/or in reaction to symptoms of malabsorption. If necessary these issues need to be offset with the use of supplements as directed by your dietician or doctor. Supplements are less affected by malabsorption of nutrients from food but their efficiency can be impacted by fast gut transit times (thus why testing is important).
Deficiencies of these vitamins and certain minerals can lead to other conditions/comorbidities, some more serious than others. For a list of the vitamins and minerals most at risk for Neuroendocrine Cancer patients, have a read of the Blog 1 - Vitamin and Mineral deficiency risks.
Thanks for listening and I remain very grateful to Tara for some assistance.
Ronny p.s. This is a big and complex subject and I only intended to cover the basics. If you need professional advice, you should speak to your doctor or dietician.
On Facebook? Please ‘Like’ my NET Cancer Blog Facebook page where I publish additional posts which will definitely be of interest to you (click here please)
On Twitter? Please follow both my accounts: @ronnyallan1 and @NETCancerBlog
On Pinterest? Please follow me here: (click here please)







