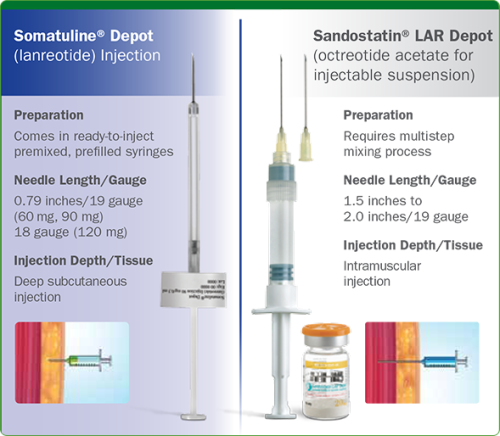
LONG ACTING LANREOTIDE (LEFT) – LONG ACTING OCTREOTIDE (RIGHT)
Somatostatin Analogues are the ‘workhorse’ treatments for those living with NETs, particularly where syndromes are involved. Although it can sometimes seem like they are only associated with serotonin releasing tumours (i.e. what might be described as Carcinoid), these types of drugs can be used to help with other NET types including Pancreatic NETs, or pNETs for short. For example, the drugs can be used for treating insulinoma, gastrinoma, glucagonoma and VIPoma (all types of pNETs). They are most effective if the NETs express somatostatin receptors.
Somatostatin is actually a naturally occurring hormone produced by the hypothalamus and some other tissues such as the pancreas and the gastrointestinal tract. However, it can only handle the normal release of hormones. When NET syndromes occur, the naturally occurring somatostatin is unable to cope. The word ‘analogue’ in the simplest of terms, means ‘manufactured’ and a somatostatin analogue is made to be able to cope with the excess secretion (in most cases).
Although there is hidden complexity, the concept of the drug is fairly simple. It can inhibit insulin, glucagon, serotonin, VIP, it can slow down bowel motility and increase absorption of fluid from the gut. It also has an inhibitory effect on growth hormone release from the pituitary gland (thus why it’s also used to treat a condition called Acromegaly). You can see why it’s a good treatment for those with NET syndromes, i.e. who suffer from the excess secretions of hormones from their NETs. Clearly there can be side effects as it also inhibits digestive enzymes which can contribute to, or exacerbate, gastro-intestinal malabsorption.
Please note somatostatin analogues are not chemo. There are two major types in use:
A frequently asked question on forums is “what is the difference between Octreotide and Lanreotide?”
Here are some interesting videos showing and explaining their administration:
This link also provides guidance on the “new formulation” Octreotide. Click here.
My own experience only includes daily injections of Octreotide (Sep-Nov 2010) and Lanreotide (Dec 2010 onwards). I’ve also had continuous infusion of Octreotide in preparation for surgical or invasive procedures over the period 2010-2012 (i.e. crisis prevention). You can read about my Lanreotide experience by clicking here. If you are interested in what might be coming downstream, please see my blog entitled ‘Somatostatin Analogues and Delivery Systems in the Pipeline’.
Thanks for listening
Ronny
Hey Guys, I’m also active on Facebook which comprises the bulk of my award-winning community. Like my page for even more news.







