One of the most discussed and sometimes confusing subjects on forums is the staging and grading of Neuroendocrine Tumours (NETs). Mixing them up is a common error and so it's important to understand the difference despite the apparent complexity.
In the most basic of terms, stage is the spread of the cancer and grade is the aggressiveness of the cancer. They are totally different things and an understanding is important as they are both critical to predict outcome (to a certain extent) and guide therapy. I'm also including information on something known as 'differentiation' as this is also a key point for NETs grading.
As patients we deal with many medical specialists during diagnosis and subsequent treatment. However, we rarely meet the pathologist who plays a critical role in the outcome. Precise diagnosis is what drives patient decisions and treatment. If the pathology is wrong, everything that follows could be incorrect as well. It's a very important area.
Staging
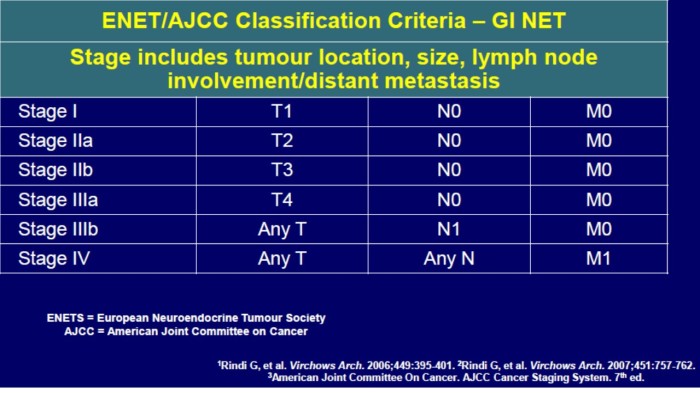
Staging is the extent or spread of disease. Most types of cancer have 4 stages, numbered from 1 to 4. Often doctors write the stage down in Roman numerals. So you may see stage 4 written down as stage IV. In addition to this standard method, there is also an agreed model known as TNM (Primary Tumour, Regional Node, Distant Metastasis) which is essentially a more detailed staging definition when combined with the Stage 1-4 model. Please note with TNM models, there could be different stage descriptions depending on the location of the primary tumour and similarly different TNM models for different tumour locations.
The following example shows the stage descriptions for a NET of the small intestine (the others are similar but worded accordingly for that part of the anatomy):
Stage 1 tumour is less than 1 cm in size and has not spread to the lymph nodes or other parts of the body
Stage 2 tumour is greater than 1 cm in size and has started to spread beyond the original location, but has not spread to the lymph nodes or other parts of the body
Stage 3 is any size tumour that has spread to nearby areas of the body and also to at least one lymph node.
Stage 4 is any size tumour that has spread to one or more lymph nodes and has also spread to other, more distant areas of the body (such as the liver).
It's also worth pointing out that Stage 4 does not necessarily mean a cancer is more dangerous than other cancers of lesser stages. This is an important point for most Neuroendocrine Cancers where Stage 4 can be apparent with a low-grade tumour i.e. Stage 4 for NETs is very often not the 'red flag' it is for other more aggressive cancers. For example, doctors may surgically remove a Stage 4 neuroendocrine tumour, while surgery might not help a patient with a different cancer in such a late stage.
Notes:
The most generic model for TNM staging is below but please note this could be adjusted for particular types of NET.
Primary Tumor (T)
TX: Primary tumor cannot be evaluated
T0: No evidence of primary tumour
Tis: in situ (abnormal cells are present but have not spread to neighbouring tissue; although not cancer, in situ may become cancer and is sometimes called preinvasive cancer)
T1, T2, T3 and T4 is a measure of the size of, and/or invasion/penetration by, the primary tumour and the wording varies between different NET sites. e.g. for a small intestinal NET:
T1 tumour invades mucosa or submucosa and size <=1 cm
T2 tumour invades muscularis propria or size >1 cm
T3 tumour invades subserosa
T4 tumour invades the visceral peritoneum (serosa)/other organs
For any T add (m) for multiple tumours
Regional Lymph Nodes (N)
NX: Regional lymph nodes cannot be evaluated
N0: No regional lymph node involvement
N1: regional lymph node metastasis
Distant Metastasis (M)
MX: Distant metastasis cannot be evaluated
M0: No distant metastasis
M1: Distant metastasis is present
Specialists can combine the Stage to create a TNM - for example:
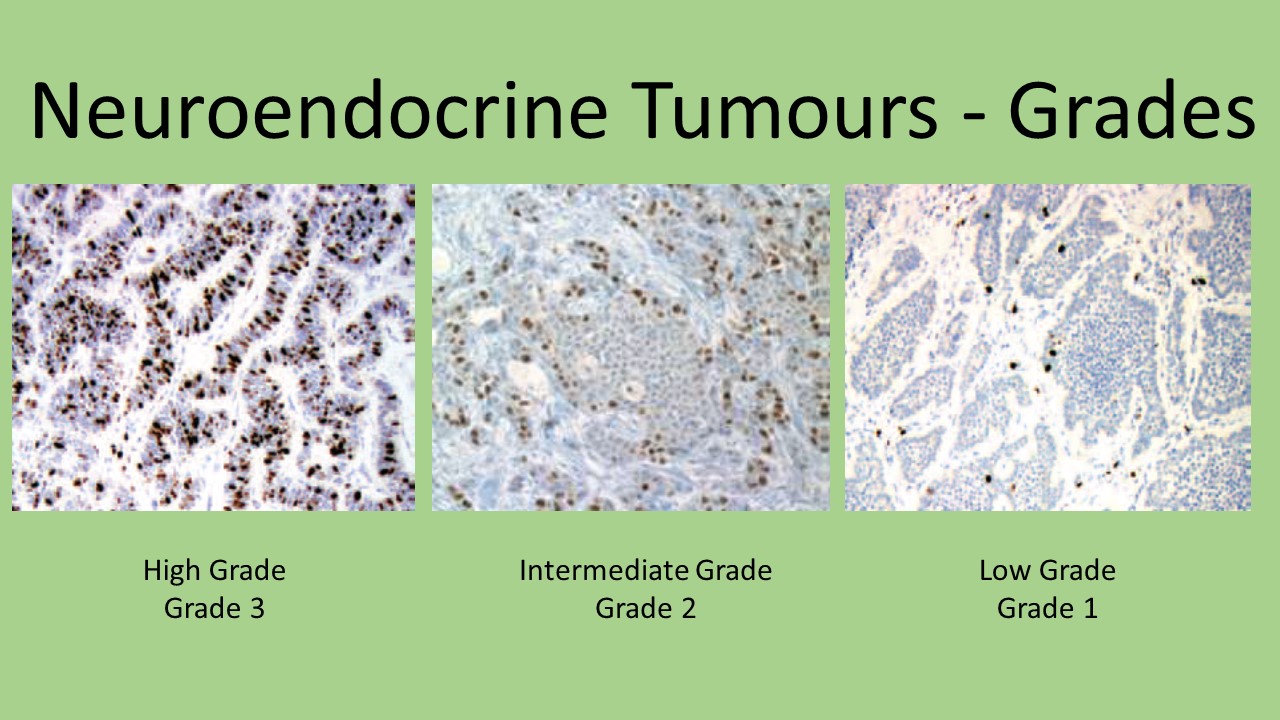
Grading and Differentiation

To understand grading, you also need to understand the concept of 'differentiation'. In the most basic of terms, 'differentiation' refers to the extent to which the cancerous cells resemble their non-cancerous counterparts. This is an important point for NETs because many low-grade tumour cells can look very similar to normal cells. Tumours fall into one of three grades based on their differentiation and their proliferative rate. The proliferative rate is measured mainly using two methods known as Miotic Count and Ki-67 index. The Ki-67 index can usually be determined, even in cases of small biopsies but Mitotic rate counting requires a moderate amount of tumour tissue (at least 50 HPFs or 10 mm) and may not be feasible for small biopsies. The Miotic Count method may be preferred or used in addition to Ki-67 for certain Lung NET scenarios as it is more helpful in distinguishing atypical from typical Carcinoid tumours, and for small and large cell lung Neuroendocrine Carcinomas.
Some of you may have heard the term 'moderately differentiated' which tended to align with an intermediate grade or Grade 2. Moderately differentiated as a classification was phased out in 2010 by WHO reducing from 3 levels to 2. Grade 2 is also defined as well differentiated but based on different proliferative rate (see table). High grade is normally referred to as Neuroendocrine Carcinoma indicating is a faster growing and more aggressive cancer.
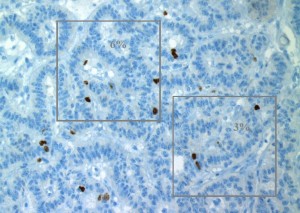
The proliferative rate can be diverse in NETs, so sampling issues can limit the accuracy of grading. More substantial samples of tumour are therefore preferable for grading thus why the Ki-67 index is preferred for biopsies where large amounts of tissue may not be available. The distinction of low-grade from intermediate grade can be challenging when using small samples.
A couple of interesting observations about NET grading which I spotted during my research and 'forum watching'. You can have multiple primary tumours and these might have different Ki-67 scores. Additionally on larger tumours, Ki-67 scores can be different on different parts of the tumour. And something I know from my own experience, secondary tumours can have higher Ki-67 scores which according to my surgeon is in keeping with a clone of the disease having become more aggressive. This raises a question which I have yet to find the answer. Is the cancer graded by the highest biopsy result regardless of primary or secondary location if proliferation results are available for both? I'll update the blog when I know :-)
This is a complex area and I hope I have condensed it sufficiently for you to understand enough for your purposes. Despite looking very scientific, it is not an exact science. There are many variables as there always are with Neuroendocrine disease. NETs can be very challenging for a pathologist even an experienced one who may not have encountered NETs before. However, it is an extremely important part of initial diagnosis and also when needed during surveillance. It is a vital tool used by Multidisciplinary Teams (MDT) in treatment plans and for prognostic purposes. If you need to learn further, I recommend
ESMO Annals of Oncology - Clinical Guidelines for Neuroendocrine gastro-entero-pancreatic tumours
Thanks for listening
Ronny
Disclaimer
My Diagnosis and Treatment History
Please ‘Like’ my NET Cancer Blog Facebook page (click here and then 'Like' the page please)







